
Your child cannot start their homework. They sit at the desk, stare at the page, sharpen the pencil three times, check their phone, and still have not written a single word an hour later. They are not being defiant. They look genuinely stuck. And you are not sure whether what you are watching is ADHD, anxiety, perfectionism, or just an overwhelming amount of work.
This confusion is extremely common among parents. And it matters. Because ADHD and situational overwhelm can look almost identical from the outside, but they have different causes, different trajectories, and very different implications for how a child should be supported.
Getting this distinction right is one of the most clinically important steps a family can take. And it is rarely possible without a proper assessment.
This article explains the key differences between ADHD and situational overwhelm due to perfectionism or workload. It helps parents understand what they are seeing, and when to seek a psychoeducational assessment.
Why This Is So Hard to Tell Apart
On the surface, ADHD and situational overwhelm produce remarkably similar behaviour.
Both can cause:
- Difficulty starting tasks
- Procrastination and avoidance
- Incomplete work
- Emotional distress around schoolwork
- Difficulty concentrating
- Forgetting instructions or deadlines
- Apparent carelessness or inconsistency
A parent watching their child struggle cannot easily tell, from behaviour alone, which is driving the difficulty. Neither can a teacher. And in many cases, the child themselves cannot tell either.
The distinction matters because the two require different responses.
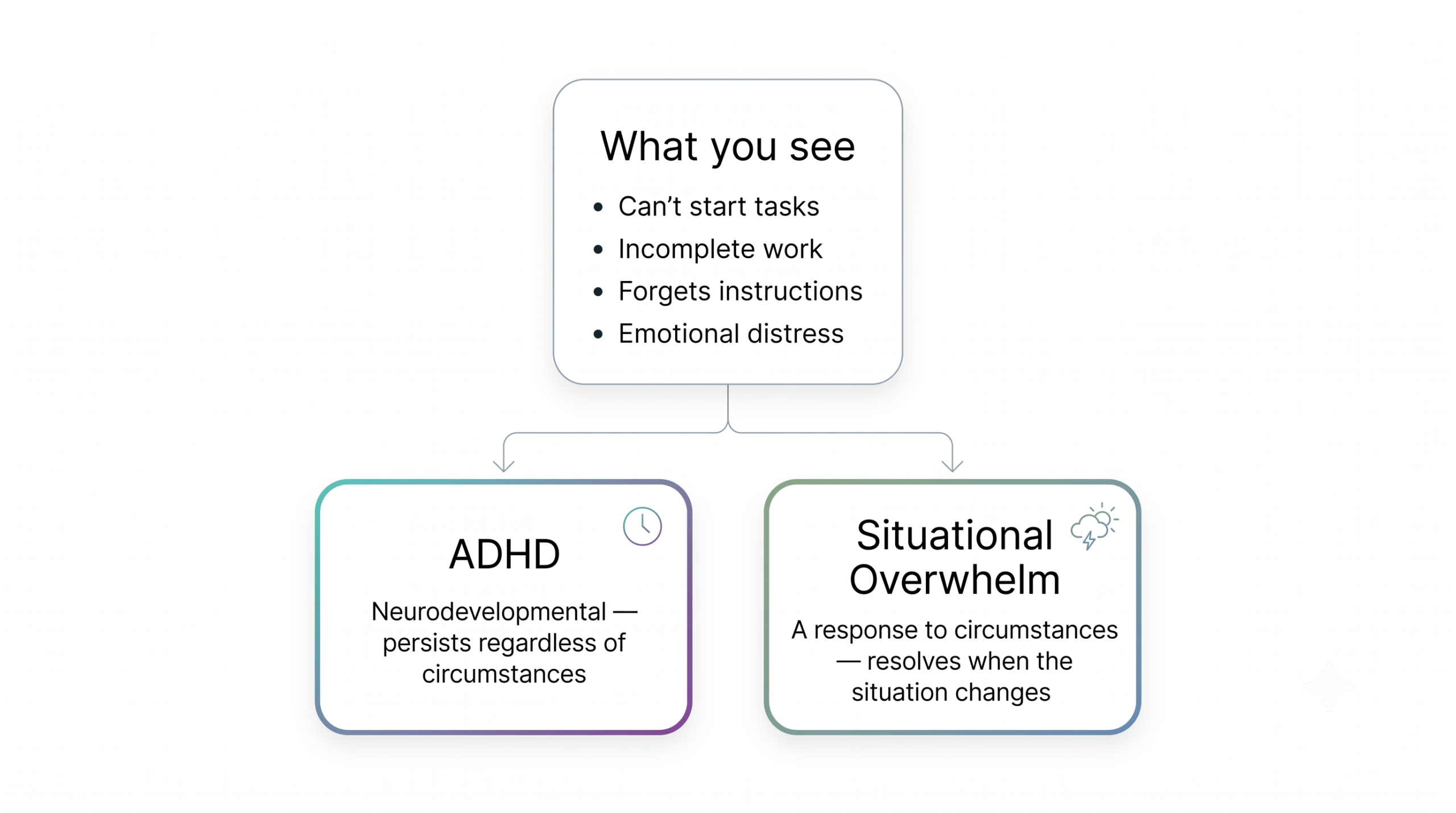
Situational overwhelm resolves when the situation changes. Reduce the workload, address the perfectionism, or support a child through a difficult transition, and the symptoms typically improve.
ADHD is a neurodevelopmental condition. It does not resolve when circumstances change. A child with ADHD will continue to struggle with attention regulation regardless of how reasonable the workload is or how relaxed the environment becomes. Without identification and appropriate support, the difficulties persist and compound.
What ADHD Actually Is
ADHD stands for Attention-Deficit Hyperactivity Disorder. Despite the name, it is not primarily about having too much energy. It is a disorder of attention regulation, impulse control, and executive functioning.
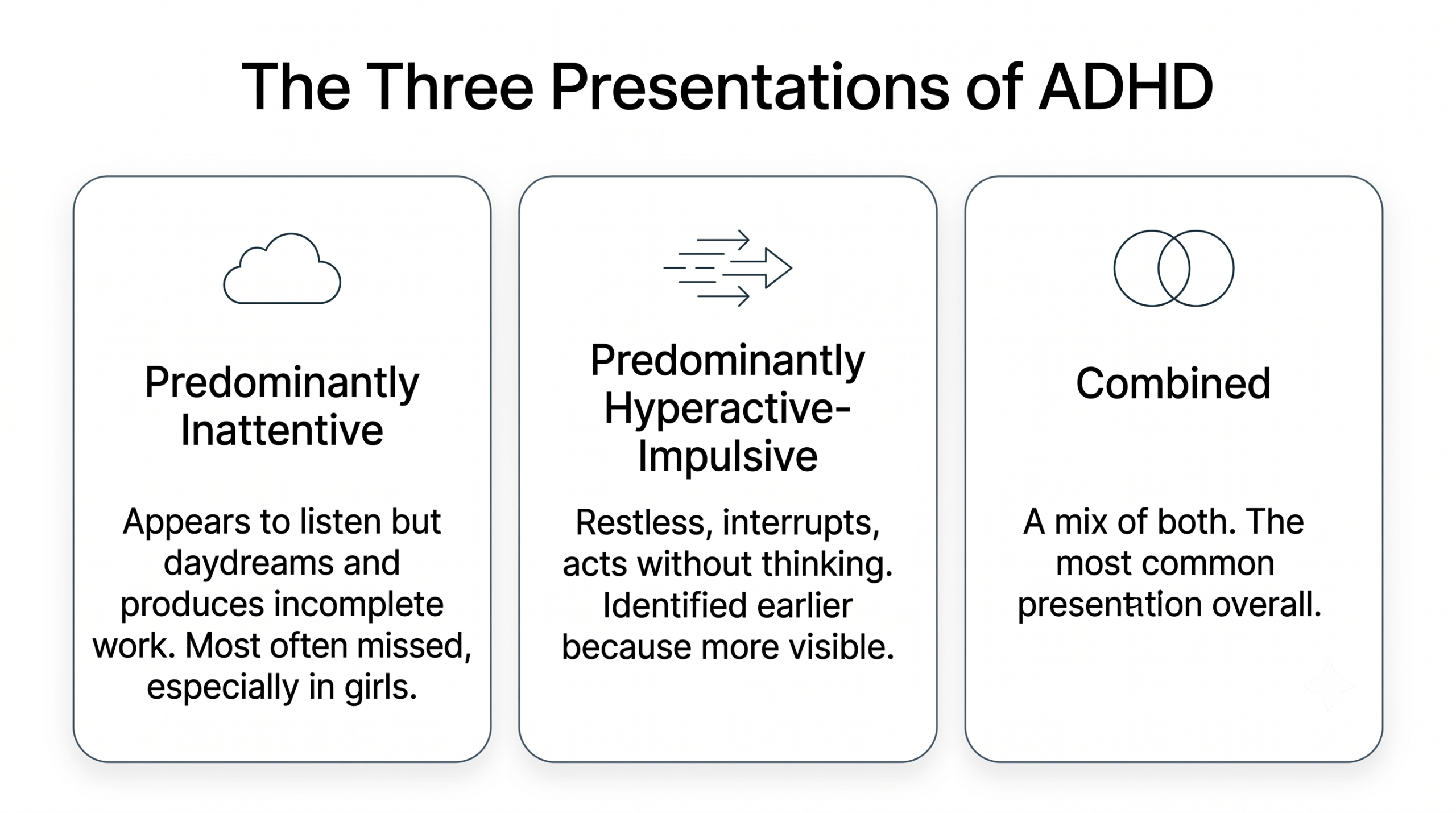
There are three presentations of ADHD:
Predominantly Inattentive
This is the presentation most commonly missed, especially in girls and in high-achieving students.
Children with inattentive ADHD appear to be paying attention but are not retaining or processing what they hear. They daydream, lose track of conversations, produce incomplete work, and appear disorganised. They are not disruptive. They are easy to overlook.
In diverse or transitional school environments, inattentive ADHD is frequently attributed to language adjustment, cultural transition, or simply being a quiet child. This delays identification by months or years.
Predominantly Hyperactive-Impulsive
This is the presentation most people picture when they hear ADHD. The child is disruptive, impulsive, and physically restless. They interrupt conversations, act without thinking, and find it genuinely difficult to stay seated.
This presentation is more likely to be identified early because it is more visible and more likely to affect the classroom environment.
Combined Presentation
Many children have a combination of inattentive and hyperactive-impulsive features. This is the most common clinical presentation overall.
What Situational Overwhelm Looks Like
Situational overwhelm describes a state in which a child’s coping capacity has been exceeded by external demands. It is not a neurodevelopmental condition. It is a response to circumstances.
In high-pressure school environments, the circumstances are frequently significant.
Perfectionism
Perfectionism is extremely common in students in high-achieving school environments. High-achieving environments, academically ambitious peer groups, and family expectations that place significant weight on academic performance, all contribute to it.
A perfectionist child does not just want to do well. They need to do it perfectly. This creates a painful bind. Starting a task means risking imperfection. So they avoid starting. Or they spend disproportionate time on one small element while the rest remains incomplete. Or they produce nothing at all because nothing they produce feels good enough.
From the outside, this looks like procrastination, avoidance, and difficulty completing work. It can look almost identical to ADHD.
The key difference is context. A perfectionist child typically struggles most with open-ended tasks, creative work, or high-stakes assignments where the standard is unclear or the possibility of failure feels significant. They may perform well under structured conditions with clear criteria.
Workload Overwhelm
Certain curricula, particularly IB, IGCSE, and AP programmes, carry significant academic demands. When a child is managing a heavy workload alongside transition stress, social adjustment, and family relocation, the cognitive and emotional load can exceed what they can sustain.
The result is a kind of shutdown. The child appears disengaged, avoidant, and unable to prioritise. Tasks pile up. Deadlines are missed. The child knows what needs to be done but cannot find a way to start.
This is not ADHD. But it can look like it. And if a child with genuine workload overwhelm is assessed at the peak of this stress, some results may temporarily resemble an attention profile.
Anxiety
Anxiety deserves particular mention because it is one of the most common sources of ADHD-like presentation in children and adolescents.
An anxious child cannot concentrate because worry is consuming cognitive bandwidth. They cannot start tasks because starting means confronting the possibility of failure. They forget instructions because their working memory is occupied with anxious rumination rather than the content of the lesson.
Anxiety and ADHD also co-occur frequently. A child can have both. This is one of the reasons clinical assessment matters so much. Without proper evaluation, it is very difficult to determine which condition is primary, which is secondary, and which treatment or support should come first.
Contexts That Make This Harder to Distinguish
Certain environments and circumstances add specific layers that complicate this distinction further.
Frequent Transitions
Children who move schools frequently experience repeated disruption to their learning routines, peer relationships, and sense of safety. This disruption can produce attention difficulties, emotional dysregulation, and avoidant behaviour that resembles ADHD.
A child who has moved schools three times in four years and is struggling to concentrate may be experiencing the cognitive and emotional effects of repeated transition rather than a neurodevelopmental attention disorder. Or they may have ADHD that has been masked until now by smaller class sizes or more accommodating environments. Or both.
Multilingual Learning
Processing academic content in a second or third language requires significantly more cognitive effort than processing in a first language. This additional load can reduce the cognitive capacity available for attention, working memory, and task completion.
A child struggling to concentrate in an English-medium classroom may be experiencing the cognitive demands of multilingual processing rather than, or in addition to, an attention disorder. Distinguishing between these possibilities requires assessment by clinicians with expertise in multilingual learning.
High-Achieving Peer Groups
Some school environments have academically ambitious peer groups. For some children, this creates a stimulating and motivating environment. For others, particularly those who are perfectionistic or anxious, it amplifies performance pressure to a level that interferes with functioning.
A child who appeared to manage well in a previous school and is suddenly struggling significantly in a more competitive environment may be experiencing a situational response to the new context rather than an emerging neurodevelopmental condition.
Key Differences: ADHD vs Situational Overwhelm
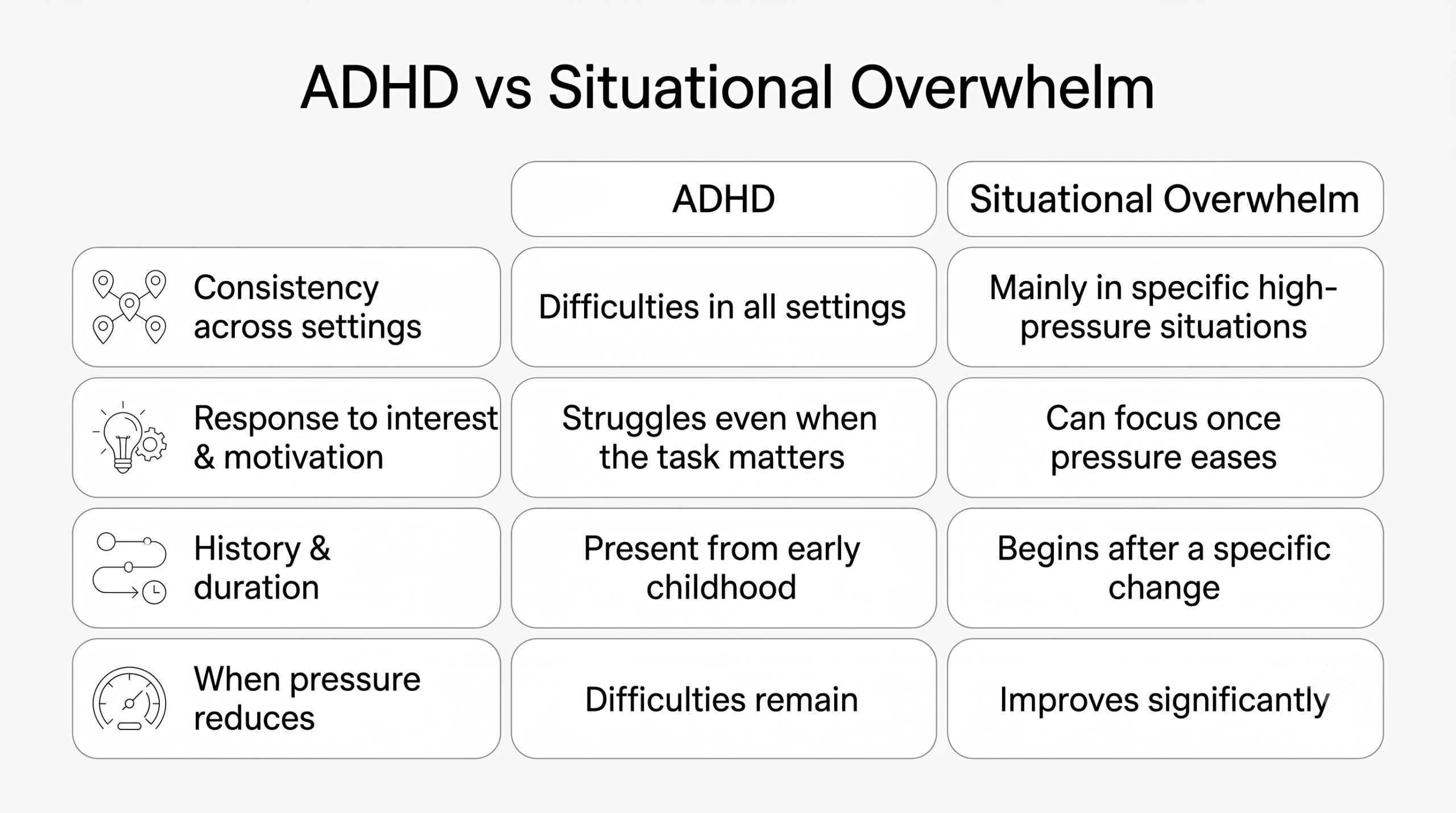
Consistency Across Settings
This is one of the most clinically useful questions to ask.
ADHD is pervasive. It affects functioning across settings regardless of the environment, the subject, or the level of interest. A child with ADHD will show attention difficulties at home, in school, in activities they do not enjoy, and in low-pressure situations.
Situational overwhelm is, by definition, situational. A child whose attention difficulties disappear on weekends, during the holidays, in extracurricular activities they love, or in subjects they find engaging is more likely to be experiencing a contextual response than a neurodevelopmental condition.
Ask yourself: Does my child struggle to focus everywhere, or mainly in specific high-pressure situations?
Response to Interest and Motivation
Children with ADHD often experience hyperfocus, an ability to concentrate intensely on activities that are highly stimulating or personally meaningful. This is not inconsistent with ADHD. In fact, it is a characteristic feature of it.
What is consistent with ADHD is the inability to sustain attention on tasks that are not inherently stimulating, even when the child understands their importance.
A child with situational overwhelm may also avoid unpleasant tasks. But they are typically able to sustain concentration on a wider range of tasks once the environmental pressure is reduced.
History and Duration
ADHD is a neurodevelopmental condition. It is present from early childhood, even if it is not identified until later.
If a child managed well for many years and the difficulties emerged following a specific change, such as a school move, a curriculum change, a significant family event, or an increase in academic demands, this suggests a situational rather than neurodevelopmental origin.
This does not mean the difficulties are less real or less serious. It means the cause is different and the response should be different.
What Happens When Pressure Reduces
Give a child with ADHD a holiday, a reduction in workload, or a change in environment, and their attention regulation difficulties remain. The context changes. The underlying condition does not.
Give a child with situational overwhelm the same relief, and you typically see significant improvement. The attention difficulties reduce. The emotional distress lessens. The child returns to something closer to their baseline functioning.
This is not always a clean test. Children with ADHD may also benefit from reduced pressure. But the degree and persistence of improvement tends to differ significantly.
When Both Are Present
ADHD and perfectionism frequently co-occur. So do ADHD and anxiety. And workload overwhelm can exist alongside genuine ADHD, making both conditions worse.
This is one of the most important reasons a proper assessment matters.
Without a comprehensive evaluation, it is not possible to determine which conditions are present, which is most significant, and what order of intervention makes clinical sense. A child who receives support for perfectionism alone, when ADHD is also present, may improve partially but continue to struggle in ways that are frustrating and confusing for everyone.
What a Psychoeducational Assessment Clarifies
A psychoeducational assessment conducted by CALM International evaluates the full picture. It does not simply screen for ADHD. It maps the child’s complete cognitive profile.
The assessment examines:
- Attention and executive functioning across multiple measures
- Working memory and processing speed
- Academic achievement relative to cognitive ability
- Emotional and behavioural functioning
- The pattern and consistency of difficulties across different domains
The findings allow our clinicians to answer specific questions.
Is what is being observed consistent with ADHD, with anxiety, with perfectionism-driven avoidance, or with a combination of these? Which is primary? What does the child need, and in what order?
For all families we assess, we also consider the child’s transition history, language background, and the specific demands of the academic environment when interpreting results. Context is not an afterthought. It is part of the clinical picture.
What Parents Can Do in the Meantime
While you are considering whether to pursue an assessment, some observations at home will be genuinely useful.
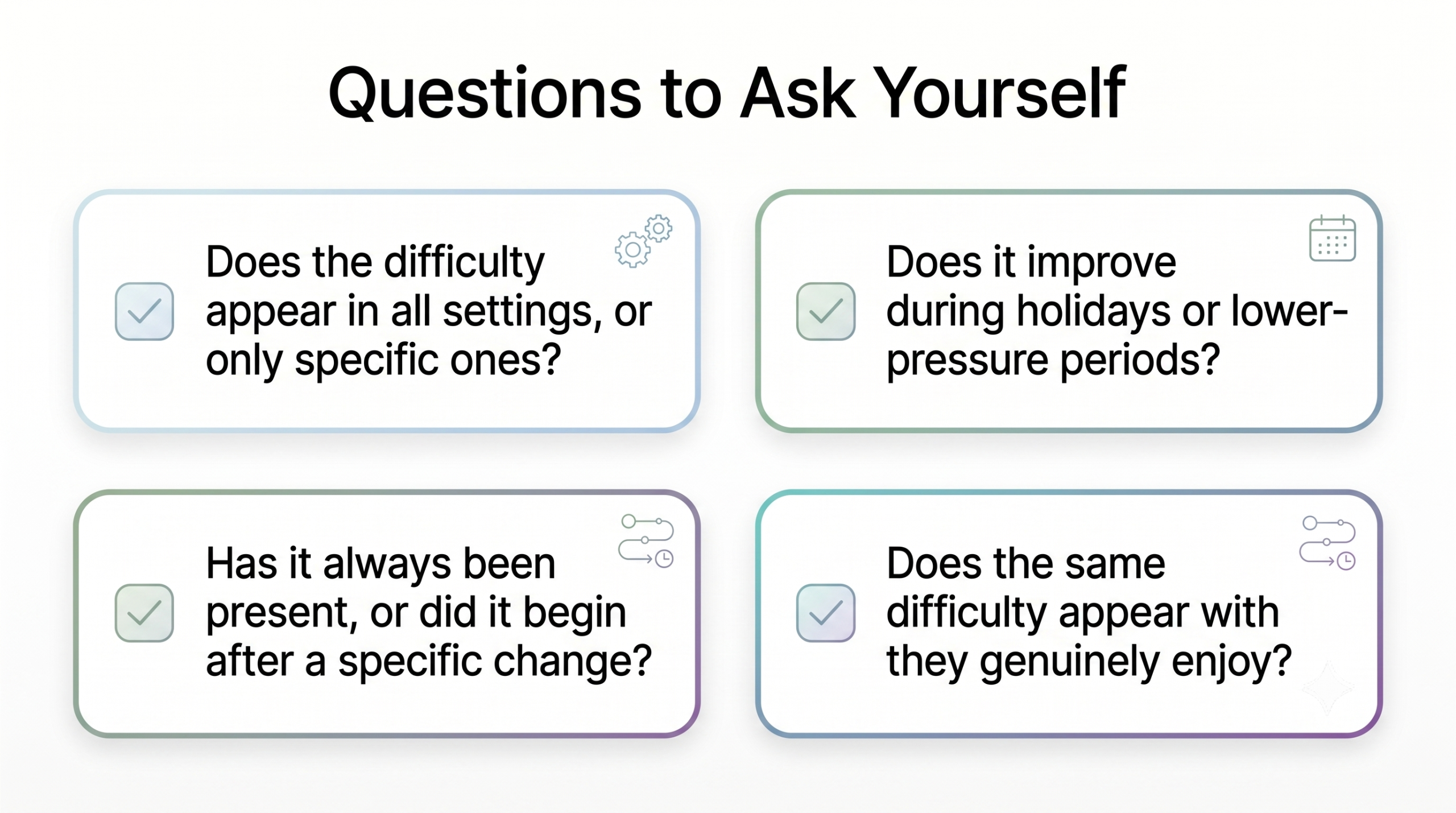
Notice and note the following:
- Does the difficulty appear in all settings or only specific ones?
- Does it improve significantly during holidays or periods of lower pressure?
- Has it always been present or did it begin after a specific change?
- Does your child show the same difficulty with activities they genuinely enjoy?
- How does your child respond when given structure, breaks, and reduced pressure?
These observations will not diagnose anything. But they will be genuinely useful information for a clinician conducting an assessment. They help distinguish between a consistent neurodevelopmental pattern and a situational response to circumstances.
If you are unsure what you are seeing, that uncertainty is itself worth taking to a clinician. Not because uncertainty means something is wrong, but because clarity is worth having.
When to Seek an Assessment
Seek a psychoeducational assessment if:
- Difficulties have been present consistently across multiple settings and over a sustained period
- Difficulties persist despite meaningful reductions in workload or pressure
- Your child is significantly more exhausted or distressed than peers in similar circumstances
- School performance is substantially below what their apparent ability would suggest
- Teachers have raised consistent concerns across multiple years
- You have a gut sense that something more is happening than ordinary adjustment
At CALM International, we work with internationally mobile families to assess children whose presentations are genuinely complex. We do not apply domestic frameworks to children whose lives and learning environments are fundamentally different. Assessment findings are interpreted in the full context of your child’s history, language background, and school environment.
If you are unsure whether an assessment is warranted, a consultation is the right first step. It costs far less than the cumulative cost of misidentification.




